Retake
A5) Incidental hepatic lesions
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with abdominal pain.
- Review the DDx considerations in a patient with abdominal pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with abdominal pain.
History
A 33-year-old female has been referred for further assessment of multiple unexpected hepatic lesions identified during a laparoscopic hernia repair. She reports no symptoms of abdominal discomfort, unexplained weight loss, fever, or vomiting. Her past medical history is significant for the use of oral contraceptives for the past 10 years. She denies alcohol consumption.
Physical Exam
Vital signs: Blood Pressure: 125/73, Heart Rate: 70, Respiratory Rate: 12, Temperature: 37ºC, Oxygen Saturation: 98%. Her BMI is 37.
Abdominal Examination: Her abdomen is soft, non-distended, and non-tender upon palpation. There is no hepatosplenomegaly, and Murphy’s sign is negative.
Labs
White blood cell count and hepatic function tests are within normal limits. Hepatic serologies are negative, and the α-fetoprotein (AFP) test is also negative.
Provisional Diagnosis
Select the Dx you believe is most appropriate
The most likely diagnosis for this patient is a hepatic adenoma, given her obesity and long-term oral contraceptive use. Hepatocellular carcinoma is less likely considering her young age, absence of known liver disease, and lack of typical symptoms. A liver abscess is unlikely due to her normal white blood cell count and absence of fever.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires routine workup and management as their condition is not immediately life-threatening.
First Imaging Study
What is the first imaging study you will order?
An abdominal MRI is an appropriate initial imaging modality to further evaluate an indeterminate liver lesion identified on an ultrasound.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
MRI Liver Mass Protocol
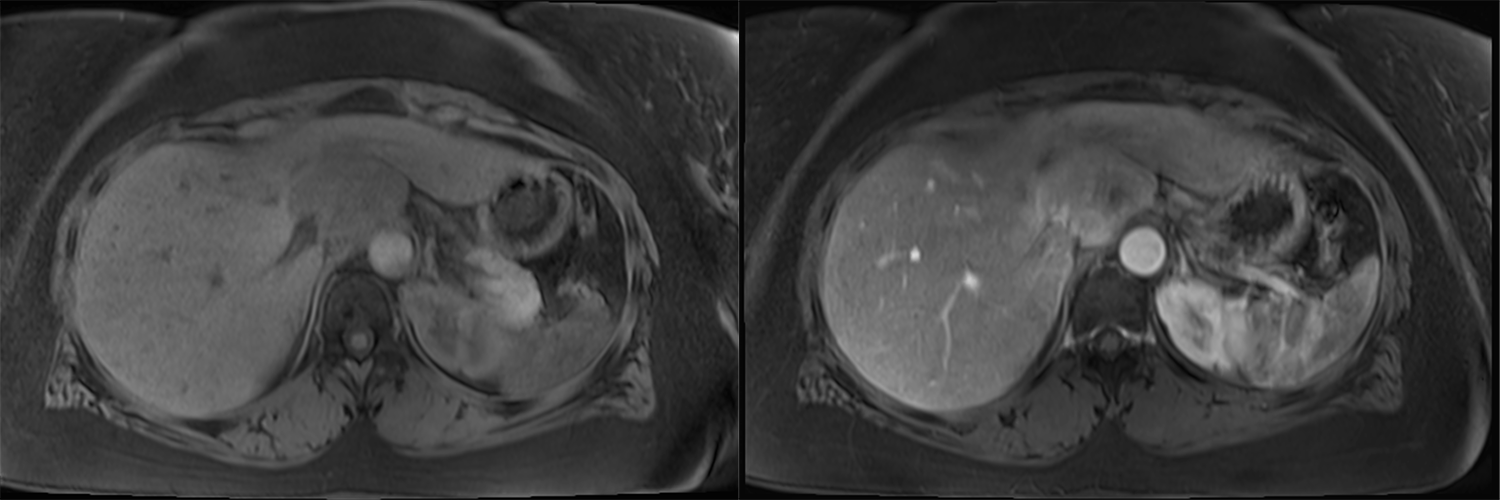
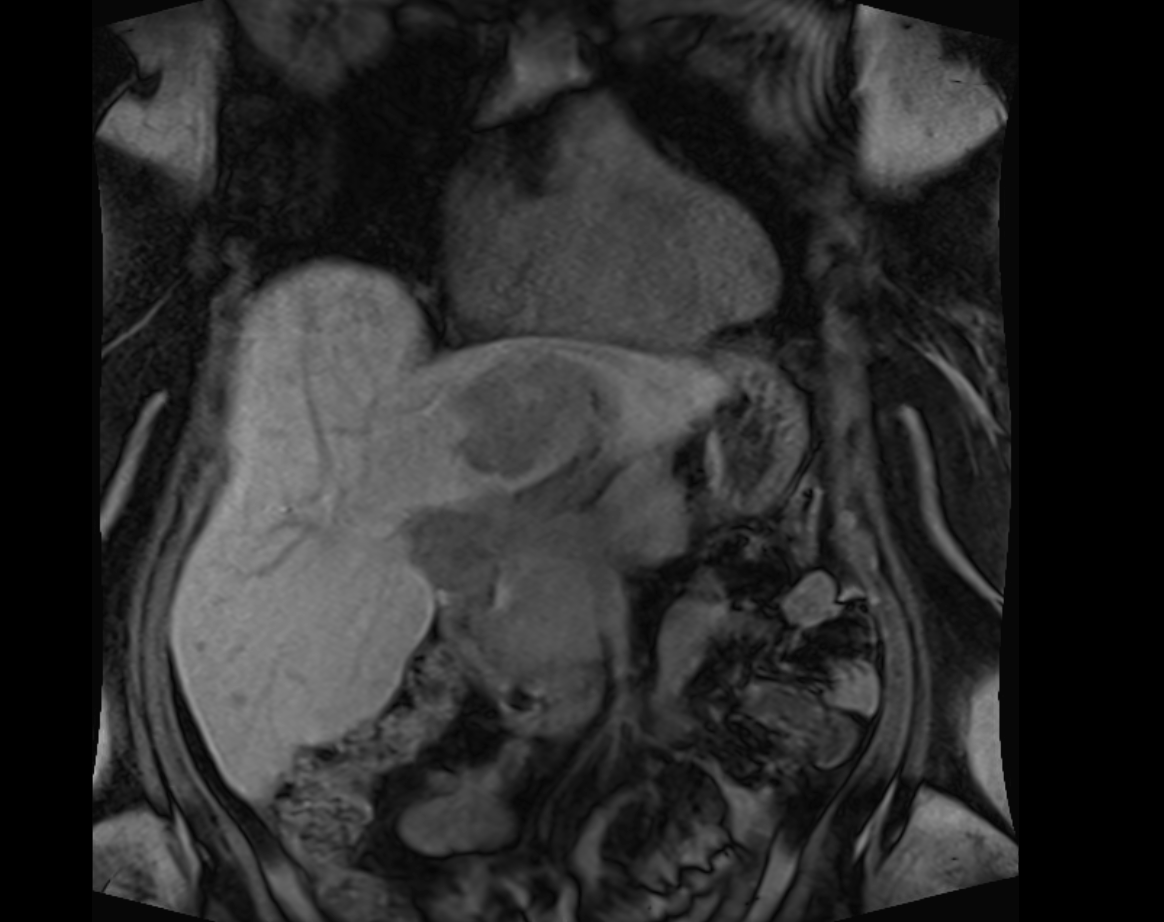
The lesion demonstrates contrast enhancement.
The lesion shows contrast enhancement, as it becomes brighter (hyperintense) after the administration of a contrast agent.
The lesion retains contrast during the hepatobiliary phase.
The lesion does not retain contrast on the hepatobiliary phase as it becomes hypointense compared to the remainder of the liver tissue on the delayed phase.
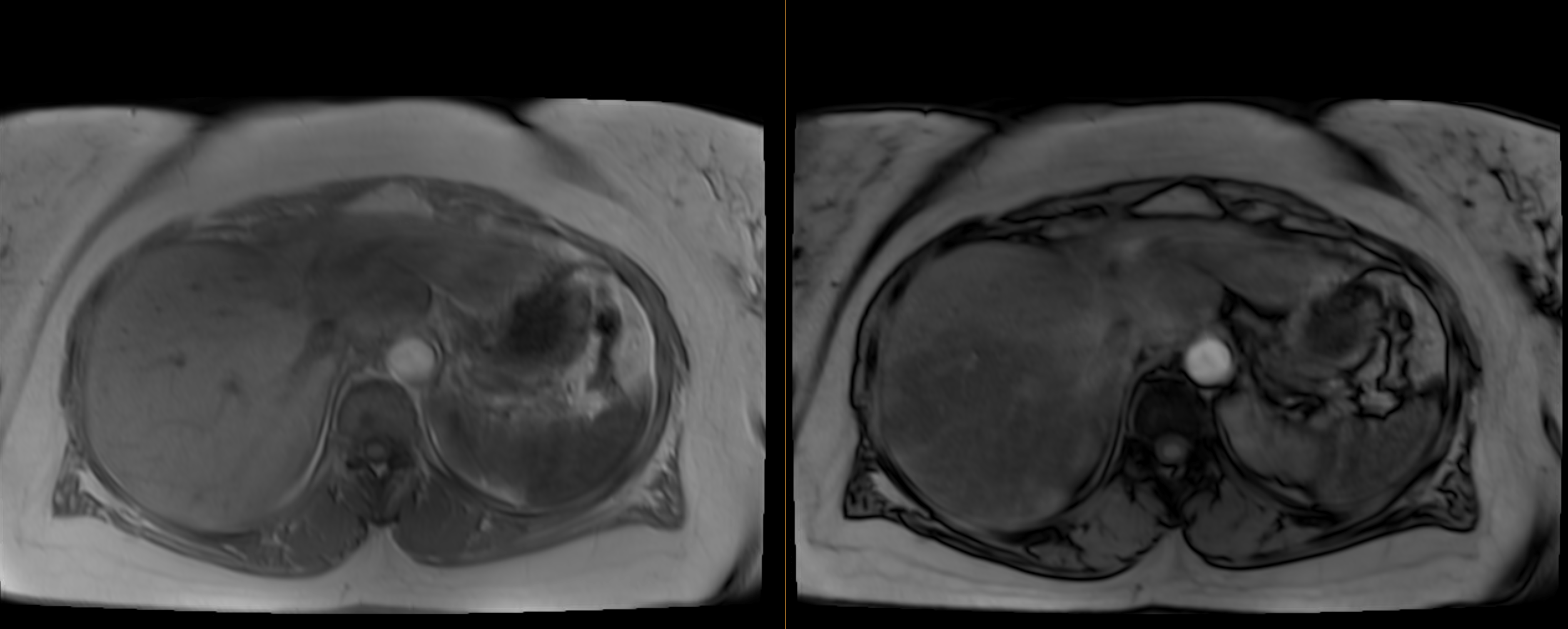
When comparing the in phase (left) and out of phase (right) images, there is evidence of:
The liver shows signal dropout, or a diffuse decrease in signal intensity in the out-of-phase image compared to the in-phase image, a characteristic suggestive of hepatic steatosis.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No further imaging is required as confirmatory imaging with MRI has already been performed.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
These arterially enhancing liver lesions, which do not retain contrast on the hepatobiliary phase, in a female with OCP use and obesity are most likely hepatic adenomas.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires routine workup and management as their condition is not immediately life-threatening.
Assessment and Plan
Please provide your assessment and plan for this patient
This is a 33-year-old obese female with a history of prolonged oral contraceptive use incidentally found to have multiple liver lesions during a laparoscopic hernia repair. An abdominal MRI highlighted multiple arterial-enhancing hepatic lesions against a backdrop of hepatic steatosis. Given the patient's history and imaging characteristics, the lesions likely represent hepatic adenomas. Due to the size and location of the largest lesion adjacent to hepatic vessels, surgical resection may not be feasible, warranting consultation with interventional radiology for potential radioembolization. Patient education should involve discussions about discontinuing oral contraceptives due to their association with hepatic adenomas. Additionally, a referral to a dietician is appropriate given her obesity.
Lessons Learned:
- Hepatocellular adenoma (HCA) is an infrequent benign, hypervascular lesion in the liver, comprised of hepatocytes and Kupffer cells.
- The formation of HCAs is often associated with factors such as the use of estrogen-rich medications, anabolic steroids, obesity, metabolic syndrome, and glycogen storage disease.
- Most HCAs are diagnosed incidentally, with abdominal discomfort being a potential presenting symptom. If ruptured, they can cause severe, potentially fatal hemorrhage.
- Appropriate imaging modalities include an ultrasound, CT, or MRI. For males, histological confirmation from surgically resected tissue is recommended.
- On an MRI, HCAs typically present as single, well-circumscribed liver lesions, exhibiting T1 contrast enhancement and T2 hyperintensity. They generally do not retain contrast in the delayed hepatobiliary phase.
- Treatment strategies generally encompass cessation of estrogen-based medications and anabolic steroids, achieving and maintaining optimal body weight, routine imaging surveillance for asymptomatic women with HCAs ≤5 cm, and surgical removal for lesions >5 cm or in all males due to risk for malignancy.
- Some lesions might regress or completely resolve.
- The risk of malignant transformation to hepatocellular carcinoma (HCC) from HCA is low. However, HCAs with beta-catenin activation present a heightened risk for evolving into HCC. Such HCAs may also imitate HCC with arterial enhancement and washout during the portal venous phase. However, cirrhosis is generally observed in HCC patients.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}